We have returned with another MyVitals Case Study! Enjoy this deep dive in our MyVitals Case Study series, where we look at different Aged Care Organisations using Provider Assist’s MyVitals software, and how they are using it to take control of their AN-ACC!
For those following along closely, you may note a common theme from our MyVitals Case Study Series to date: the importance of an effective Reclassification strategy for the successful clinical management of your facilities. Reclassifications are fundamental to ensuring you are funded well for the care you are delivering.
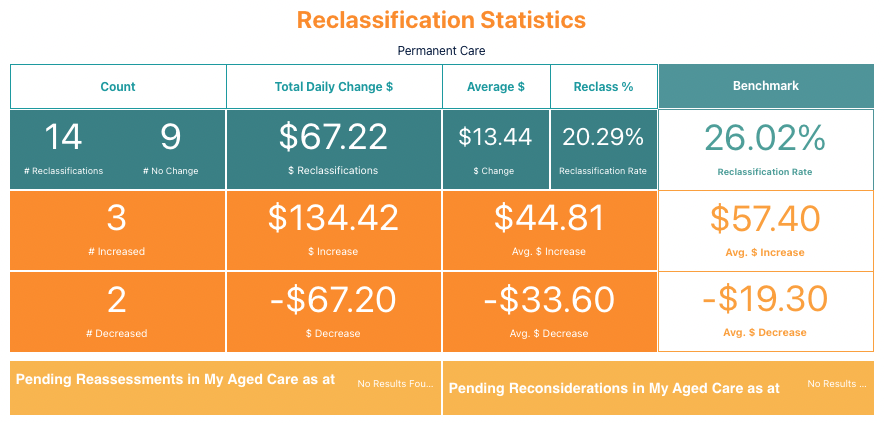
Let’s look at a facility’s Reclassification statistics since the transition to AN-ACC on the 1/10/2022.
The Good News:
- 14 Reclassifications
- 22% of their residents have been reclassified since Oct 1 – exceeded the Industry benchmark by over 3%
- resulting in an additional $67.22 per day for the facility.
Room for Improvement:
- only 3 Reclassifications resulted in increased funding.
- 9 Reclassifications resulting in no change
- 2 Reclassifications resulting in a decrease.
It is a lot of effort to prepare for a resident for reclassification, so it is important to ensure the resident receives the outcome that is consistent with their care and to safeguard against decreases.
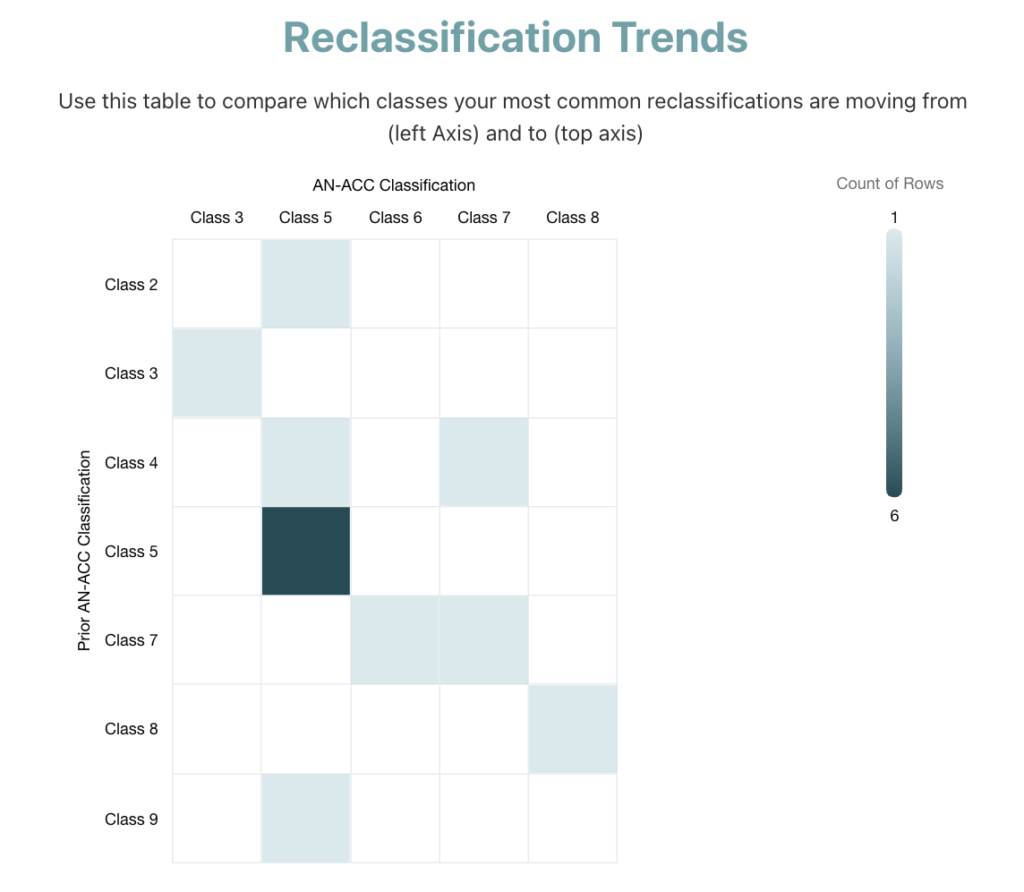
How to identify a non-ideal Reclassification outcome?
MyVitals includes a heatmap that demonstrates the outcomes of completed Reclassifications. This allows us to investigate the Reclassification program at an individual resident level and see the outcomes for each Reclassification.
What can this facility do to improve their Reclassification performance?
Firstly, it is important to consider a Reclassification from the perspective of the AN-ACC Assessor processes. There are three sources of clinical information an Assessor can draw upon:
- The clinical documentation.
- The care staff
- The resident
This forms a triangulating approach for assessment, where the Assessor should place equal weighting on each category, but we know they often don’t. It’s important your clinical story is congruent across all 3 areas, so no matter where the Assessor places their attention, they will come to the same conclusion, or you can utilise Reconsideration processes. An unexpected Reclassification outcome can occur where:
- There is incongruency in this information, usually from gaps in clinical assessment, documentation and care planning processes.
- Gaps in AN-ACC knowledge in those selecting residents for Reclassification, or those preparing the assessments, documentation & care plans.
- Not utilising the Reconsideration process where you disagree with the outcome.
To investigate what this looks like in practice, let’s consider a Resident named Betty. She entered care 12 months ago and received a Class 2 AN-ACC. Since entering care, her mobility has declined following a fall, and now she requires extra assistance from a walking frame and the care staff. Based on this decline in Betty’s mobility, the care staff have identified that her care needs are no longer being catered for by her classification and have projected she could be a Class 4 or higher.
Betty will tell the Assessors that she can still do cartwheels like when she was 12, so it is important to ensure that her clinical documentation and the care staff are aligned for the resident’s care needs.
Of course, we can’t control exactly how the Assessors conduct their assessments. Where an Assessor favours resident interview, this will result in a non-ideal outcome in this scenario. An effective Reclassification process will identify that this outcome is incorrect and utilise Reconsideration avenues.
Lessons Learnt
This example demonstrates how we can use the dashboards in MyVitals to analyse our Reclassification performance. Despite this facility seeing an increase in funding from their Reclassification efforts, they are currently experiencing a low success rate for achieving increased funding through Reclassifications. This is typified where nearly half of their Reclassifications have been requested for Class 5 residents and resulted in no change. It highlights shortcomings for the facility’s clinical processes where the projected outcomes for residents are not being adequately met. One main area of significance for this facility that is differentiating to AN-ACC Assessors, is that a resident is medium-cognition instead of high-cognition.
By understanding this gap, we can remedy this by placing greater focus and providing extra attention to these Reclassifications in the future. If all these residents submitted for Reclassification received the expected outcomes, the facility could receive upwards of $350/day in addition to the $134.72/day they achieved. This would equate to $182,500 in annual funding, which indicates the importance of successfully meeting outcomes projected in a Reclassification process.
This would only be possible with an effective Reclassification strategy, where the facility is confident in the story that is provided by their clinical documentation, care staff and the resident. In doing this, the facility makes the most of the effort they are putting into Reclassifications and enables them to provide the best possible care for their residents.
Have you seen the other articles in our MyVitals Case Study series?
See how different Aged Care Providers use Provider Assist’s MyVitals software to have visibility into and take control of their AN-ACC!
If you would like to find out more about MyVitals and book a demo – simply head here! https://go.providerassist.com.au/bookyourmyvitalsdemo

Connor Chrisfield
Reporting & Data Analyst